
-
Shoulder Stabilization Surgeon in California
Frequent dislocations of the shoulder joint can lead to chronic shoulder instability. Surgery to stabilize the shoulder may be recommended when conservative treatment options fail. Dr. Nassos provides diagnosis and individualized nonoperative and operative treatments for the shoulder including shoulder stabilization in California. Dr. Nassos also provides the highest level of care during and after surgery. Contact Dr. Nassos’s office for an appointment today!
Disease Overview
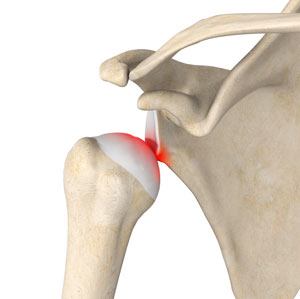
Shoulder instability is a chronic condition that causes frequent dislocation of the shoulder joint. A dislocation occurs when the end of the humerus (the ball portion) partially or completely dislocates from the glenoid (the socket portion) of the shoulder. A partial dislocation is referred to as a subluxation while a complete separation is referred to as a dislocation. The repeated dislocation of the humerus out of its socket is called chronic shoulder instability. A tear in the labrum or rotator cuff and a ligament tear in the front of the shoulder (a Bankart lesion) may lead to repeated shoulder dislocations.
Indications for Shoulder Stabilization
When conservative treatment options such as medications, rest and ice application fail to relieve shoulder instability, your surgeon may recommend shoulder stabilization surgery.
Shoulder Stabilization Surgery Procedure
Shoulder stabilization surgery is performed to improve stability and function to the shoulder joint and prevent recurrent dislocations. It can be performed arthroscopically, depending on your particular condition, with much smaller incisions. Arthroscopic stabilization is a surgical procedure to treat chronic instability of the shoulder joint.
Arthroscopy is a minimally invasive surgery and is performed through two tiny incisions (portals), about half-inch in length, made around the joint area. Through one of the incisions, an arthroscope (small fiber-optic viewing instrument) is passed. A television camera attached to the arthroscope displays the images of the inside of the joint on the television monitor, which allows your surgeon to view the cartilage, ligaments and the rotator cuff while performing the procedure. A sterile saline solution is pumped into the joint, which expands it and provides a clearer view. Bone spurs, defects or tissue tears will be identified.
Your surgeon makes use of tiny surgical instruments that are passed through the other incisions to treat the condition. Any tear in the rotator cuff will be sutured or stapled. The sutures will be held in place with the help of a small anchor that is drilled into the upper part of the humerus. Further, a thermal shrinkage device may be used in order to make the ligaments tight and prevent instability.
Postoperative Care for Shoulder Stabilization
Following the procedure, your surgeon may advise the use of a continuous passive motion machine to prevent stiffness and improve the range of motion of the shoulder joint. Pain medications will be prescribed to keep you comfortable. A shoulder sling can be worn for 4-6 weeks to immobilize and facilitate healing. A postoperative rehabilitation program including strengthening exercises will be advised for 6-9 months. You will be able to participate in sports in about 18 to 36 weeks after the surgery.
Advantages of Shoulder Stabilization
The major benefits of arthroscopic stabilization as compared to the open repair are that it gives a chance to identify and treat coexisting diseases, lesser pain and complications, combined with a shorter hospital stay.
Risks and Complications of Shoulder Stabilization
As with any surgical procedure, there may be certain risks and complications involved and include infection of the surgical wound, post-operative stiffness, risk of arthritis, muscle weakness and injury to the nerves and blood vessels.
If you would like additional information on the treatment of shoulder conditions or would like to learn more about shoulder stabilization surgery, please contact Dr. Nassos, serving the communities of California.